Hair Pulling and Emotional Avoidance: What Comes First?

May 30th, 2022
Online test
Find out the severity of your symptoms with this free online test
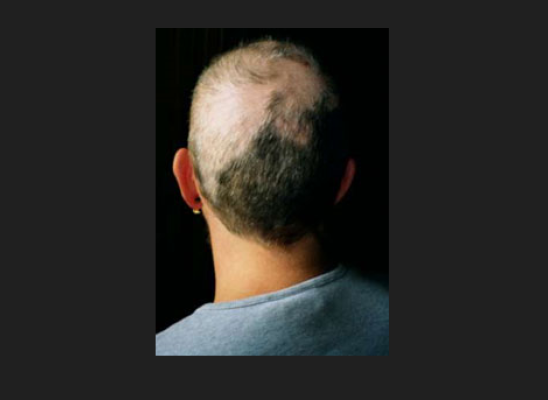
Trichotillomania (TTM) is a body-focused repetitive disorder (BFRB) characterized by repetitive hair pulling that results in noticeable hair loss. Just why someone might engage in hair pulling is not well-understood. TTM is highly heterogeneous meaning that there is significant variation among people who live with TTM. How they pull, when and why they pull, and even the areas of the body where they pull varies quite a bit.
While the exact cause of TTM is unknown, it is thought that certain behavioral and cognitive factors play a role in its development and perpetuation. Among the many antecedents (internal experiences that precede hair pulling) that have been mentioned in the literature as contributing to the development and exacerbation of BFRBs include negative affective states such as anxiety, sadness or boredom, emotional reactivity, stress, trauma, perceptual sensitivity…the list goes on. Hair pulling is thought to be an attempt to reduce or avoid unpleasant, negative feelings or sensations. It’s a phenomenon that is seen in other mental health disorders as well as TTM.
Experiential avoidance is engaging in unhealthy behaviors to escape or avoid unpleasant internal psychological experiences (e.g., fear, anxiety). These tactics may be effective in the short term, but do not eliminate the source of the discomfort. Over time, the response, in this case hair pulling, becomes habitual and the person’s “go-to” response. Some studies have found that experiential avoidance is related to the severity of TTM, suggesting that it may be the mediator between those internal experiences and the hair-pulling severity but that relationship is unclear.
When research answers one question, it opens the door for more. Are all antecedent experiences to hair pulling the same? Are they about avoidance or something else? A 2020 study took a closer look at the antecedents of hair pulling and the role of experiential avoidance in TTM.
Antecedents and TTM Severity
People describe their antecedent experiences in many different ways. Are all the experiences uniquely different or do they represent experiences with common themes or characteristics? One of the goals of the study was to further define and categorize antecedent experiences beyond the existing literature. Responses from participants were varied, as expected. Five broad categories of antecedents to pulling emerged:
- Bodily sensations
- Physical symptoms
- Mental anxiety
- General uncomfortableness
- Thoughts, ideas, and images
General uncomfortableness was the most frequently cited antecedent to hair pulling, followed by bodily sensations, physical symptoms, mental anxiety, and thoughts, ideas, and images. These results seemed to be consistent regardless of the person’s preferred area to pull hair from.
The study authors did note that while mental anxiety was not the most frequently cited experience, it may still be a prominent feature. Anxiety is closely associated with TTM. Some of the results here may be more about how the person experiences or defines their anxiety or feelings of uncomfortableness. Some of the respondents may have chosen “uncomfortableness” as their way of describing what might also be considered anxiety.
Experiential Avoidance
Another objective of the study was to understand more about the relationship between various antecedent experiences and emotional avoidance. Four of the five classes of antecedents were associated with higher levels of experiential avoidance:
- Bodily sensations
- Physical symptoms
- Mental anxiety
- General uncomfortableness
Thoughts, ideas, and images did not show a significant association with experiential avoidance.
Only general uncomfortableness was associated with higher levels of severity of TTM. Based on the results of the study, emotional avoidance was not found to be a mediator between antecedent experiences and TTM severity.
Putting It All Together
The study’s findings build on previous research and further describe the intricate relationship between one’s internal experiences, emotional avoidance, and how their role in the severity of TTM. Internal experiences are more than cognitions and include experiences of things like sensations and images and mental anxiety. Based on the cognitive-behavioral model, thoughts, feelings and behavior all interact with each other to shape behavior. The findings support the idea that bodily sensations and emotions like anxiety play a key role in the behavior of hair-pulling.
The variation in internal experiences reported by participants speaks adds to the voices advocating treatment that is personalized. Understanding how internal experiences may affect hair pulling may help to shape the treatment of TTM. Treatment for trichotillomania is a lifelong process unique to every individual and requires an understanding of your unique needs. Identifying a person’s antecedent experiences may be a way to serve as an “early warning system” and act as a cue to try alternative coping strategies.
Given the role of emotional avoidance in hair pulling, acceptance-based therapies such as Acceptance and Commitment Therapy (ACT) and Dialectical Behavior Therapy (DBT) may be helpful in treating hair pulling. Because emotional avoidance is associated with many antecedent experiences, therapy that allows for contact with the distressing experience may offer an opportunity to create a response other than pulling hair.
Both ACT and DBT, when combined with Habit Reversal Training (HRT) have been shown to reduce hair pulling. ACT as a stand-alone treatment has also been shown to be helpful in reducing hair pulling with outcomes similar to HRT-enhanced with ACT.
So, which comes first, hair pulling or emotional avoidance? The jury is still out on that answer. Given the cyclical nature of repetitive, habitual behavior, the answer may lie in both/and. In the meantime, researchers continue to learn more about TTM, and hope remains for effective, individualized treatments.
References
1. Franklin, M. E., Zagrabbe, K., & Benavides, K. L. (2011). Trichotillomania and its treatment: a review and recommendations. Expert review of neurotherapeutics, 11(8), 1165–1174. https://doi.org/10.1586/ern.11.93
2. Norberg, M. M., Wetterneck, C. T., Woods, D. W., & Conelea, C. A. (2007). Experiential avoidance as a mediator of relationships between cognitions and hair-pulling severity. Behavior Modification, 31(4), 367-381. https://www.researchgate.net/publication/6287162_Experiential_Avoidance_as_a_Mediator_of_Relationships_Between_Cognitions_and_Hair-Pulling_Severity
3. Wetterneck, C., Singh, R. S., & Woods, D. W. (2020). Hair pulling antecedents in trichotillomania: Their relationship with experiential avoidance. Bulletin of the Menninger Clinic, 84(1), 35–52. https://doi.org/10.1521/bumc_2020_84_01
4. Lee, E. B., Homan, K. J., Morrison, K. L., Ong, C. W., Levin, M. E., & Twohig, M. P. (2018). Acceptance and commitment therapy for trichotillomania: A randomized controlled trial of adults and adolescents. Behavior Modification, 44(1), 70-91. doi:10.1177/0145445518794366
Online test
Find out the severity of your symptoms with this free online test



Start your journey with TrichStop
Take control of your life and find freedom from hair pulling through professional therapy and evidence-based behavioral techniques.
Start Now